As a healthcare provider, you deliver timely, effective, and compassionate care in the high-stakes settings of emergency departments and cardiology units, managing complex cases under the constraints of limited resources and time pressures.
The High Stakes of Cardiac Care
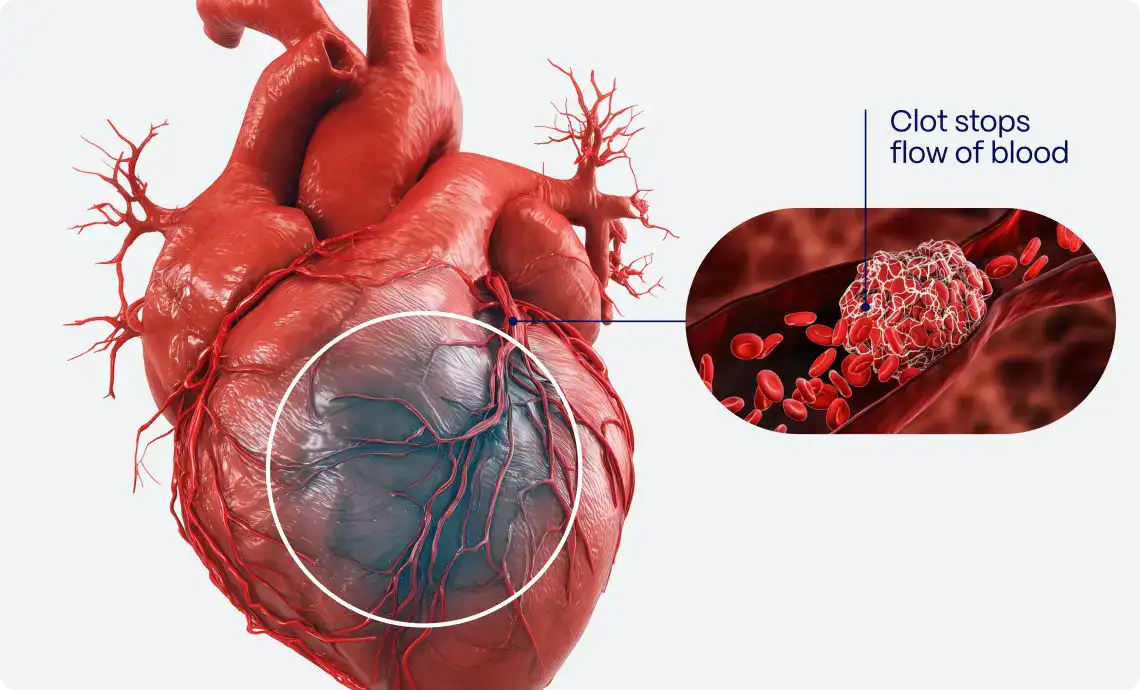
Chest pain, the most common symptom in patients presenting to ED1, is at the heart of your clinical decision-making. Each year, over 50 million patients come to EDs with chest pain. With only 10% of these cases due to ACS1, identifying it can be like finding a needle in a haystack. However, with 4 million cases involving ACS1, the stakes are extraordinarily high, emphasizing the need for optimal patient outcomes.
Addressing Clinical Challenges Head-On
Managing ACS is highly challenging due to a 40% rate of false positive STEMI diagnoses, leading to unnecessary cath lab activations2 and underdiagnosis of acute coronary occlusions. One-third of patients presumed to be NSTEMI, actually suffer from occlusive coronary lesions requiring immediate interventions3. The oversight in this category includes failing to recognize STEMI-equivalent patterns, which, although not presenting with classic ST-elevation, still signify critical coronary artery occlusions.
The current rule-in pathway for early identification of STEMI patients is suboptimal, leading to frequent misidentification, wasted resources, and significant physician burnout. This inefficiency results in an average of $135,000 per year in canceled cath lab activation costs (assuming $1,500/cancellation) per mid-high volume center. Diagnostic inaccuracies expose patients to risks from unwarranted or delayed procedures, extend hospital stays, and worsen outcomes, with an average delay of 10.35 hours in time to coronary angiography and a doubling of the one-year all-cause mortality rate. Additionally, these issues strain healthcare resources and contribute to an 18.2% annual turnover rate among healthcare professionals4.
PMcardio for Organisation: Transformative Advances in Cardiac Medicine
PMcardio for Organizations is a diagnostic platform developed not just to serve as another tool in our kit but to revolutionize how you approach the chest pain patient’s journey from the moment they enter your facility. Designed by clinicians for clinicians, PMcardio is undergoing extensive validation by a network of over 35 leading international clinical research institutions and its effectiveness has been documented in more than 10 peer-reviewed medical publications.

PMcardio harnesses the power of its OMI AI ECG Interpretation model, setting a new standard in the rapid assessment and triaging of chest pain patients, having screened over 400,000 ECGs since its launch and being utilized by more than 48,000 healthcare professionals worldwide.
Its impact was demonstrated at the Cardiovascular Centre Aalst in Belgium, among other sites, where the implementation of PMcardio achieved:
- 68% reduction in false positive STEMI alerts and second opinion consultation requests
- 100% sensitivity in true positive STEMI patients
- 34% reduction in ECG to balloon time for STEMI patients, speeding up critical interventions
- 50% decrease in door-to-ECG time month-over-month, with twice as many patients receiving ECG recordings within the guideline window
- 56% decrease in door-to-balloon time for NSTEMI-OMI

PMcardio’s effectiveness is further validated by leading institutions:
- Uniklinik Köln: Achieved 97% specificity in unselected all-comer chest pain patients without ST elevation
- Cardiocentro Ticino, Lugano, Switzerland: Demonstrated a 73% positive predictive value in out-of-hospital cardiac arrest (OHCA) patients without ST elevation
- SSM Health St. Louis University, MO: Showed twice the sensitivity compared to cardiologists
- Hennepin County Medical Center, MN: Realized a 58% reduction in false positive cath lab activations
- Stony Brook Medicine, NY: Attained 74% sensitivity in detecting acute OMI
These findings reveal how the platform can help you achieve more accurate diagnoses, streamline patient triage, and improve workflow processes.
Aligning Diagnostic Excellence Across the Board
Accurately diagnosing acute coronary occlusions is complicated by variable diagnostic skills and the rapidly evolving understanding of ECG patterns. Pattern recognition in ECG interpretation requires extensive hours of learning, which is often not feasible for physicians, especially emergency medicine doctors, who must stay proficient in many fields. As medical knowledge and diagnostic criteria evolve, keeping pace with advancements becomes increasingly challenging6.
PMcardio addresses this need effectively by standardizing diagnostic processes using AI algorithms trained on over 2.5 million patient contacts across 32 geographically distinct locations. This training is designed to standardize care and minimize bias, making the PMcardio OMI AI ECG model robust across age, sex, and ethnic subgroups, while also ensuring transparency and explainability.
At the optimal threshold, the PMcardio OMI AI ECG model exhibited a significantly higher sensitivity in identifying OMI compared with STEMI criteria, achieving 81% versus 32.5%5.

PMcardio offers a level of diagnostic security that outpaces even seasoned medical professionals. Despite initial concerns that the OMI paradigm shift might increase cath lab activations, the absolute number of activations is actually lower because many false positives are prevented. This means fewer unnecessary procedures, reduced patient risk, and more appropriate use of cath labs. Consequently, interventional cardiologists are only called for relevant patients.


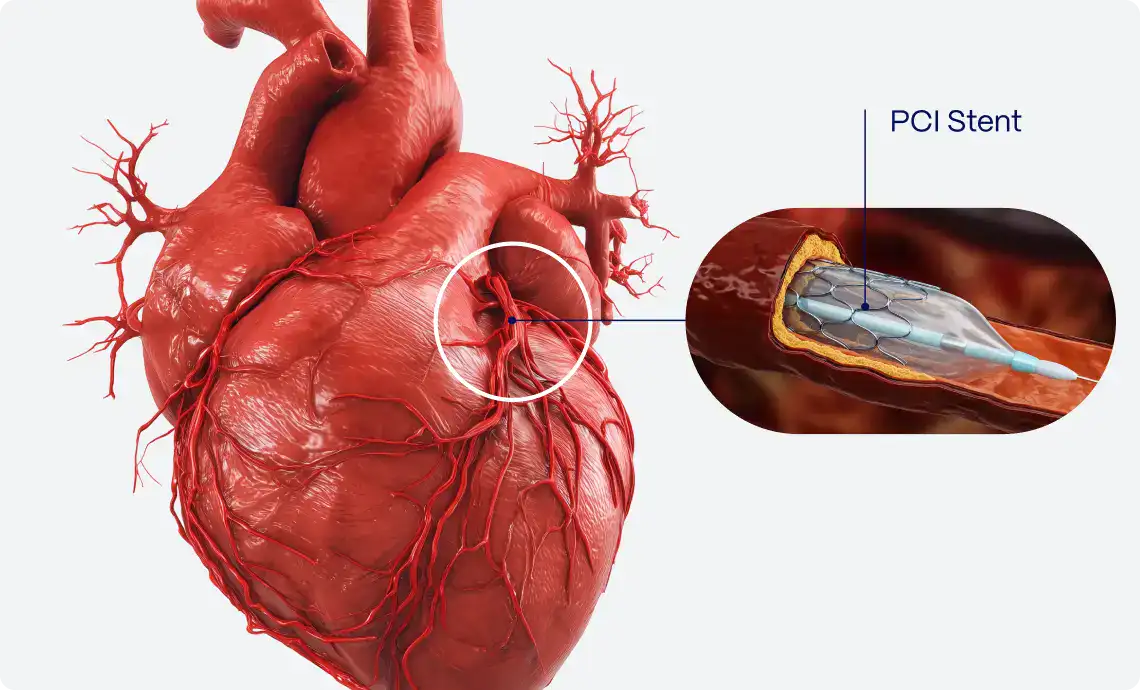
Effective Triage that Speeds Up Diagnoses and Cath Lab Activations
PMcardio optimizes the triage process, significantly accelerating diagnoses and cath lab activations for critical cases from the first point of contact. The platform utilizes advanced ECG processing technology to substantially shorten the time from symptom onset to treatment by reducing the ECG to balloon time for STEMI patients by one-third. PMcardio makes it more attainable to meet the crucial 90-minute window from first medical contact as recommended by ACC/ESC/AHA guidelines to prevent irreversible myocardial damage7, contributing to a decrease in PCI time for patients with STEMI equivalents by an average of 10.3 hours, enhancing the efficiency of care5.
As the platform enables immediate cardiology overreads, it further eliminates the delays traditionally associated with seeking second opinions or coordinating with cardiovascular specialists across the hospital.
Out-of-Hours Made Easier
PMcardio’s impact goes beyond daytime operations, addressing the high demands of out-of-hours cath lab activations. By significantly reducing false positive STEMI alerts and unnecessary activations, it minimizes callouts and optimizes cath lab resources. This efficiency allows healthcare staff to focus on real emergencies.
PMcardio’s mobile accessibility enables healthcare professionals to access ECG data and make decisions remotely, even from home. This flexibility ensures continuity of care during out-of-hours, potentially increasing rest periods and reducing burnout among medical teams, leading to a more balanced workload and improved well-being for hospital staff.
Empowering Nursing Staff
PMcardio’s all-in-one design maximizes accessibility and efficiency, as it is readily available on various devices such as smartphones and tablets. This mobility ensures that critical patient information and diagnostic tools are always at the nurses’ fingertips, no matter where they are in the hospital. This not only accelerates the decision-making process but also bolsters nurses’ competence, enabling them to act decisively and confidently. By enhancing their responsiveness in critical situations, PMcardio aims to improve patient advocacy and reinforce nurses’ empowerment in their clinical roles.

Streamlining Workflows
Effective communication among nurses, emergency medicine physicians, and cardiologists is essential, yet often challenged by the fast-paced, high-stress environment of emergency care and varying clinical perspectives. PMcardio for Organizations offers a personalized and unified care-coordination platform that delivers real-time diagnostic interpretations accessible to the entire team. This shared platform supports simultaneous access for improved decision-making, promoting quick alignment on treatment strategies and speedy referrals.
The flexibility of PMcardio for Organizations allows it to be tailored to the specific needs of each team member, whether on a personal, ward-specific, or institutional level. It can be configured to match the unique workflows of different departments, ensuring that the ECG review process is as smooth as possible, regardless of the clinical setting.
A Tool That Understands Clinical Needs
Developed with direct input from seasoned medical professionals, PMcardio addresses the real-world complexities of managing chest pain in a high-pressure environment. It doesn’t just add to the noise; it cuts through it with precision and speed, enhancing your capabilities and allowing you to focus more on what matters most – patient care.

Commitment to Privacy and Clinical Excellence
PMcardio for Organizations allows for precise diagnostic assessments based solely on ECG data, without the need to identify the patient. While the secure platform stores ECG records to support ongoing management, it ensures that personal patient details remain confidential, prioritizing privacy alongside effective clinical decision-making in full compliance with security and privacy regulations8. The platform also features enterprise-level functionalities that enable safe and integrated patient management, including central report management through a single admin dashboard, where all ECGs within your organization can be accessed and reviewed.
Additionally, PMcardio for Organizations enhances the capabilities of your team to detect trends, refine treatment protocols, and support educational activities. Implement this tool in your preparations for mortality and morbidity meetings, participation in grand rounds, and during discussions at quality improvement and clinical governance meetings to make your sessions more data-driven and effective.
As you embark on this new era in STEMI patient care with PMcardio for Organizations, the platform stands as your partner in mastering the complexities of modern healthcare, ensuring that every patient benefits from top-tier, timely care.
Book a Demo to see how PMcardio for Organizations can transform chest pain patient’s journey at your facility.
References
- Rui P, Kang K. National Hospital Ambulatory Medical Care Survey: 2017 emergency department summary tables. National Center for Health Statistics. Available from https://www.cdc.gov/nchs/data/nhamcs/web_tables/2017_ed_web_tables-508.pdf.
- Larson DM, Menssen KM, Sharkey SW, et al. “False-Positive” Cardiac Catheterization Laboratory Activation Among Patients With Suspected ST-Segment Elevation Myocardial Infarction. JAMA. 2007;298(23):2754-2760. doi:10.1001/jama.298.23.2754.
- Khan AR, Golwala H, Tripathi A, Bin Abdulhak AA, Bavishi C, Riaz H, et al. Impact of total coronary occlusion on outcomes of patients with non-ST-elevation myocardial infarction undergoing percutaneous coronary intervention: A systematic review and meta-analysis. Eur Heart J. 2017 Dec 21;38(43):3082-3089. doi: 10.1093/eurheartj/ehx391. PMID: 29020244.
- Taking the Heart Team Staffing Business Seriously. Diagnostic and Interventional Cardiology. Available from: https://www.dicardiology.com/article/taking-heart-team-staffing-business-seriously
- Herman R, Smith SW, Meyers HP, Bertolone DT, Leone A, Bermpeis K, et al. Poor prognosis of total culprit artery occlusion in patients presenting with NSTEMI. Eur Heart J. 2023 Nov;44(Suppl_2):ehad655.1536. doi: 10.1093/eurheartj/ehad655.1536.
- Wagner GS, Macfarlane P, Wellens H, Josephson M, Gorgels A, Mirvis DM, et al. AHA scientific statement: standardization and interpretation of the electrocardiogram. J Am Heart Assoc. 2013 Jul 24;2(4):e000268.
- Gulati M, Levy PD, Mukherjee D, Amsterdam E, Bhatt DL, Birtcher KK, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021 Nov 30;144(22):e368-e454. doi: 10.1161/CIR.0000000000001029. Epub 2021 Oct 28. Erratum in: Circulation. 2021 Nov 30;144(22):e455. Erratum in: Circulation. 2023 Dec 12;148(24):e281. PMID: 34709879.
- Powerful Medical. Available from: https://www.powerfulmedical.com