50% of heart attacks do not meet classic ECG-based STEMI criteria
What this means in practice
A substantial proportion of patients with a life-threatening heart attacks do not show classic ST-segment elevation on their first ECG. Despite having an acutely blocked coronary artery that would benefit from urgent reperfusion, these patients are often not recognized as high-risk at first medical contact.
Contemporary studies consistently show that 30–50% of patients with an occluded culprit artery do not meet traditional STEMI criteria at presentation [2]. As a result, many patients with ongoing myocardial ischemia are initially triaged as “NSTEMI” or “non-diagnostic ECG,” delaying escalation of care.
Why this happens
Gold-standard STEMI triage at first medical contact based on international guidelines relies on fixed millimeter thresholds of ST-segment elevation.
While effective for many patients, this approach has important limitations:
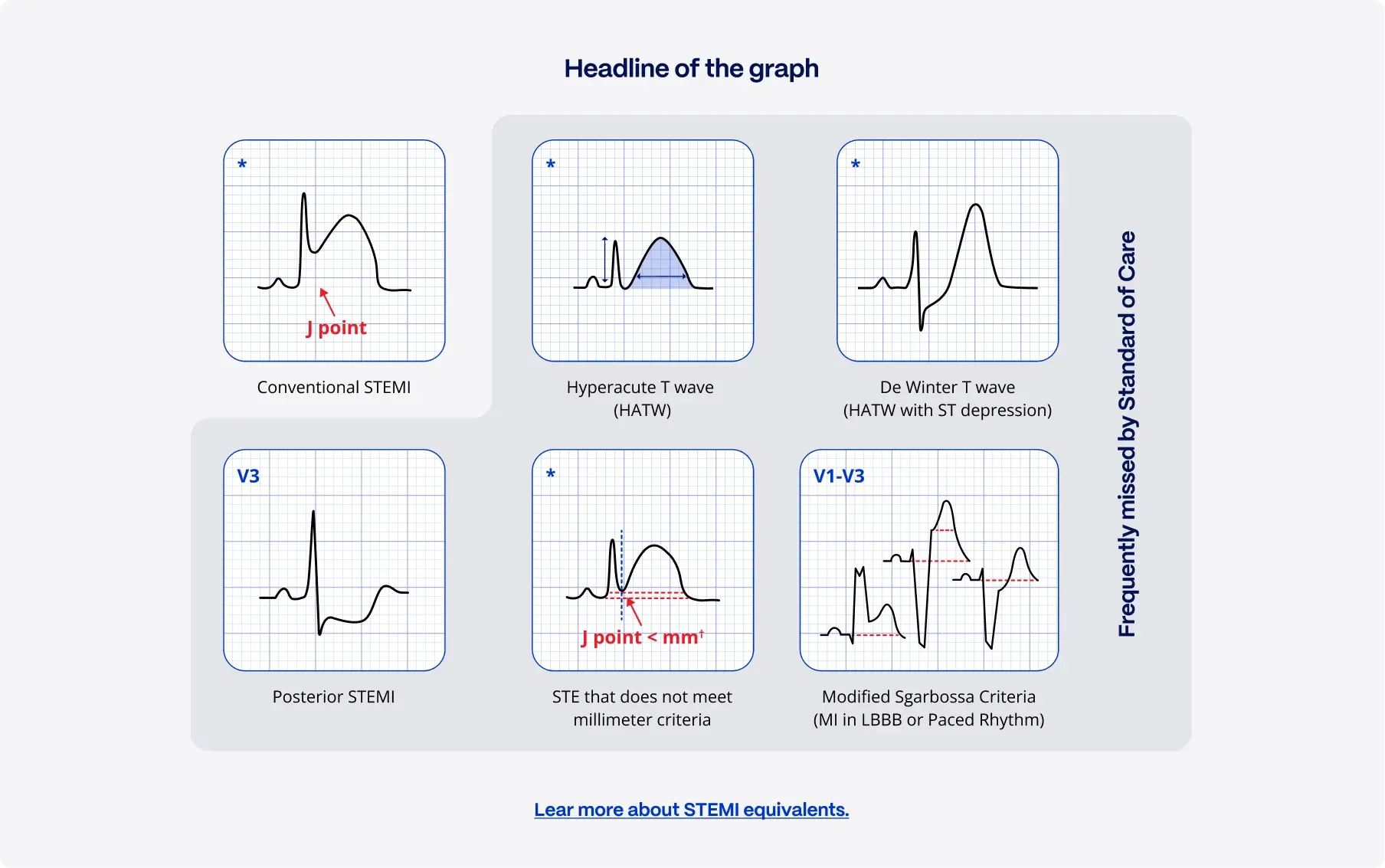
- Acute heart attacks frequently present with subtle ST-segment changes, hyperacute T-waves, posterior patterns, or proportional ECG changes that fall below guideline cutoffs
- First ECGs may be recorded before ST-elevation fully develops (hyperacute presentations)
- Certain infarct locations, particularly left circumflex or posterior infarctions, do not lead to ST-elevation on standard 12-lead ECGs
These ECGs are often labeled as “NSTEMI” or “equivocal,” despite representing the same time-critical pathology as classic STEMI.
Clinical consequences
Delays to invasive management
Patients with occlusive myocardial infarction without STEMI criteria experience significantly longer times to coronary angiography, often 4–5 hours later than patients with classic STEMI. Many are only “ruled in” after repeat ECGs, rising biomarkers, or clinical deterioration. [1]
Worse clinical outcomes
Multiple observational studies have shown that patients with an occluded artery who do not meet STEMI criteria have:
- Larger infarct size
- Higher short- and long-term mortality
- Increased incidence of heart failure
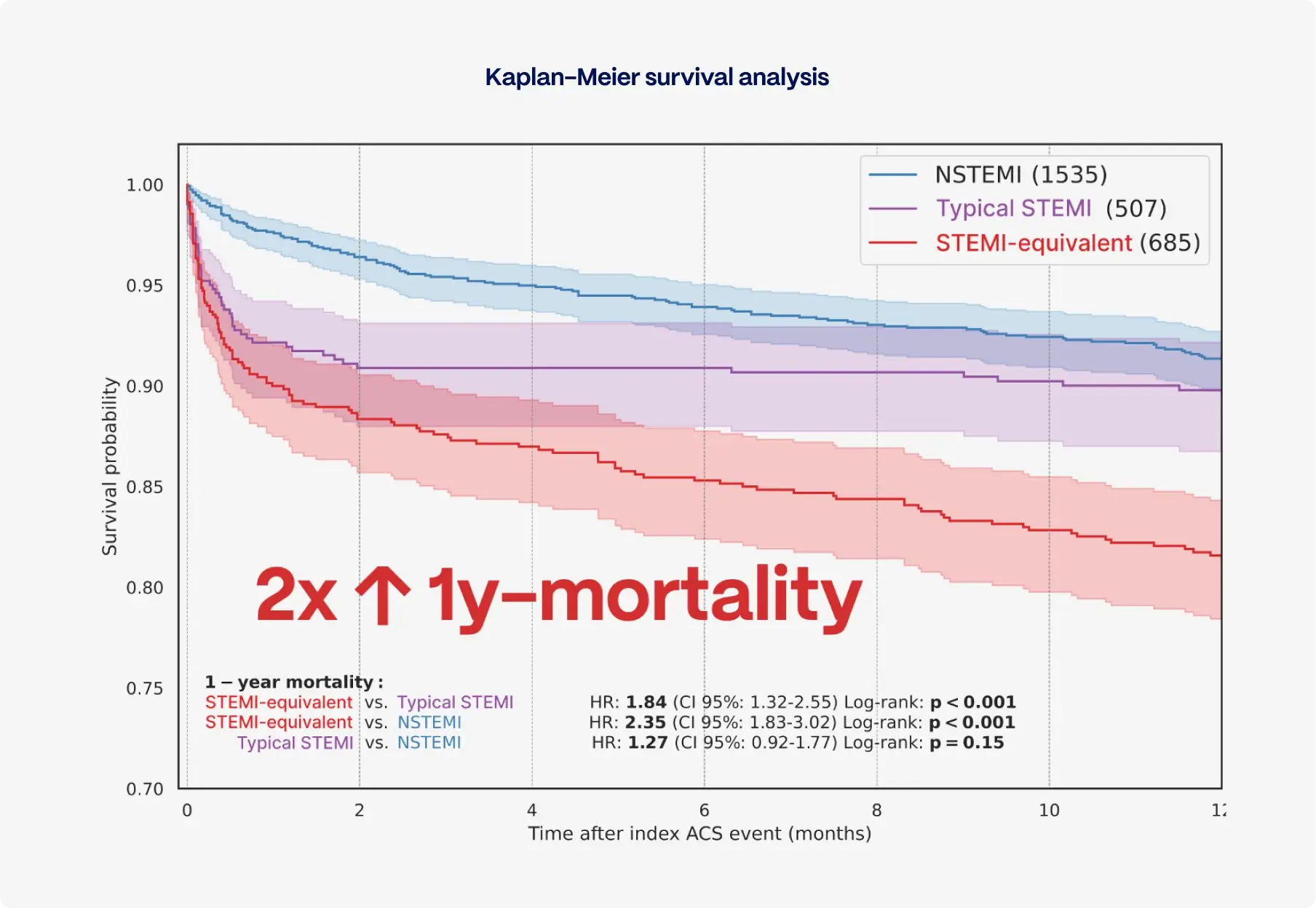
In pooled analyses, these patients have been shown to experience nearly double the mortality compared with patients without coronary occlusion, despite often being younger and having fewer comorbidities.
Gap between guidelines and real-world practice
Although clinical guidelines recommend early invasive management for NSTEMI patients with high-risk features, real-world adherence remains limited. In practice, only about 6% of NSTEMI patients who meet high-risk criteria receive early invasive management within guideline-recommended timeframes. [3]
This highlights a critical reality: once patients are classified as “Not a STEMI,” escalation of care is frequently delayed, even when ongoing ischemia is present.
- [1] Khan AR, Golwala H, Tripathi A, Bin Abdulhak AA, Bavishi C, Riaz H, Mallipedi V, Pandey A, Bhatt DL. Impact of total occlusion of culprit artery in acute non-ST elevation myocardial infarction: a systematic review and meta-analysis. Eur Heart J. 2017 Nov 1;38(41):3082-3089. doi: 10.1093/eurheartj/ehx418. PMID: 29020244.
- [2] Jollis JG, Granger CB, Zègre-Hemsey JK, Henry TD, Goyal A, Tamis-Holland JE, Roettig ML, Ali MJ, French WJ, Poudel R, Zhao J, Stone RH, Jacobs AK. Treatment Time and In-Hospital Mortality Among Patients With ST-Segment Elevation Myocardial Infarction, 2018-2021. JAMA. 2022 Nov 22;328(20):2033-2040. doi: 10.1001/jama.2022.20149. PMID: 36335474; PMCID: PMC9638953.
- [3] Lupu L, Taha L, Banai A, Shmueli H, Borohovitz A, Matetzky S, Gabarin M, Shuvy M, Beigel R, Orvin K, Minha S, Shacham Y, Banai S, Glikson M, Asher E. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardial infarction patients. Clin Cardiol. 2022 Apr;45(4):359-369. doi: 10.1002/clc.23781. Epub 2022 Mar 9. PMID: 35266561; PMCID: PMC9019882.