Occlusion Myocardial Infarction: A Revolution in Acutecoronary Syndrome

Overview
The 2025 ACC Guideline for the Management of Patients With Acute Coronary Syndromes claims that “Patients with NSTEMI may have a partially occluded coronary artery leading to subendocardial ischemia, while those with STEMI typically have a completely occluded vessel leading to transmural myocardial ischemia and infarction.” This is accompanied by a visual representation of a partially occlusive thrombus labeled ‘NSTEMI’ above an electrocardiogram (ECG) showing ST depression and T wave inversion, and a completely occlusive thrombus labeled ‘STEMI’ above an ECG showing ST elevation. This paradigm has remained despite two decades of angiographic and evidence-based ECG advances, which highlight the multiple reasons why a revolution in acute coronary syndrome (ACS) is needed, and has begun.
Key findings
- Critiques the 2025 ACC ACS guideline's STEMI/NSTEMI paradigm.
- Argues occlusion MI (OMI) better reflects angiographic evidence.
- Calls for evidence-based ECG diagnosis after two decades of advances.
Published in: Advances in Interventional Cardiology
Published on: 19 May 2025
Background
The STEMI/NSTEMI paradigm has long guided diagnosis and management: STEMI is assumed to correspond to a fully occluded artery and warrants emergent reperfusion, while NSTEMI is considered non-occlusive.
However, angiographic data over recent decades challenge this neat separation: a substantial fraction of patients classified as NSTEMI in fact have total occlusion of a culprit coronary vessel, and these patients have worse prognoses compared to non-occlusive NSTEMIs.
The authors note a “no false negative paradox” inherent in the classic paradigm, because patients without ST elevation but with occlusion are simply labeled NSTEMI, and false negatives are hidden in classification.
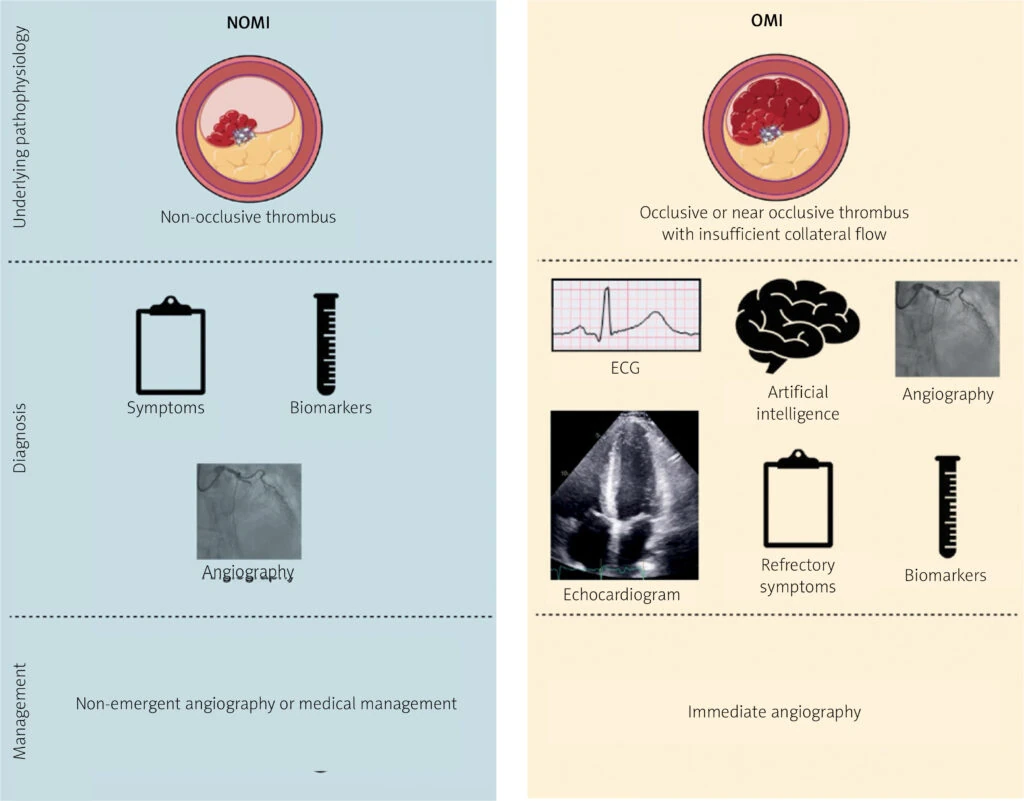
To remedy this, in 2018, the “OMI Manifesto” was proposed, promoting a paradigm based on the presence or absence of acute coronary occlusion (or near-occlusion with insufficient collateral flow), regardless of whether ST elevation is present.
The authors assert that advances in ECG interpretation (including recognition of subtle signs like hyperacute T waves, ST depression in reciprocal leads, modifications in bundle branch block, etc.) and artificial intelligence make more sensitive detection of OMI feasible.
Methods
Because this is an editorial rather than an original research study, the “methods” are argumentative and literature-based rather than experimental. The authors:
Call for adoption of AI and systemic changes (e.g. registry definitions, quality metrics) to advance the OMI paradigm in real clinical care.
Review and synthesize existing angiographic and meta-analytic evidence on rates of coronary occlusion among patients without classic ST elevation.
Critique the limitations of the STEMI/NSTEMI paradigm and its entrenched influence on quality metrics and guideline approaches.
Present the concept of the OMI paradigm and survey supporting evidence, including studies where ECG reading under the OMI paradigm improved sensitivity without sacrificing specificity.
Illustrate specific ECG patterns that may portend occlusion despite the absence of ST elevation (e.g., hyperacute T waves, reciprocal changes, modified Sgarbossa criteria, etc.).
Results
Meta-analyses show that ~ 25–34 % of NSTEMI patients may harbor complete culprit artery occlusion, and that such patients have significantly worse outcomes than NSTEMI patients without occlusion.
Classic STEMI ECG criteria have limited sensitivity: pooled estimates suggest sensitivity as low as ~ 43.6 % for detecting acute coronary occlusion.
Advanced ECG interpretation under the OMI approach (including recognition of non-classic ECG patterns) has demonstrated improved sensitivity for detecting occlusion while maintaining specificity. For example, in prior studies, blinded readers using OMI criteria nearly doubled sensitivity for acute coronary occlusion compared to STEMI criteria.
The editorial also cites work showing that OMI vs. non-OMI classification better predicts mortality than STEMI vs. NSTEMI classification.
AI-based ECG models are emerging as promising tools to detect subtle ECG changes consistent with occlusion.
Conclusion
The authors conclude that the STEMI/NSTEMI paradigm is no longer sufficient and often misclassifies patients, thereby delaying or denying timely reperfusion to many true occlusions. The OMI concept reframes ACS classification around pathophysiology (occlusion) rather than rigid ECG thresholds. By applying refined ECG criteria, integrating AI, and changing guideline and quality metric frameworks, clinicians can better identify and treat patients at risk. The authors call for adoption of OMI in future ACS research, registries, clinical practice, and policy.
Authors: William H. Frick,Jesse TT McLaren,H. Pendell Meyers,Stephen W. Smith
Share this article
About PMcardio
PMcardio is the market leader in AI-powered diagnostics, addressing the world’s leading cause of death – cardiovascular diseases. The innovative clinical assistant empowers healthcare professionals to detect up to 40 cardiovascular diseases. In the form of a smartphone application, the certified Class IIb medical device interprets any 12-lead ECG image in under 5 seconds to provide accurate diagnoses and individualized treatment recommendations tailored to each patient.
About Powerful Medical
Powerful Medical leads one of the most important shifts in modern medicine by augmenting human-made clinical decisions with artificial intelligence. Our primary focus is on cardiovascular diseases, the world’s leading cause of death.
Established in 2017, Powerful Medical has embarked on a mission to revolutionize the diagnosis and treatment of cardiovascular diseases. We are a medical company backed by 28 world-class cardiologists and led by our expert Scientific Board with decades of experience in daily patient care, clinical research, and medical devices. The results of our research are implemented, developed, certified, and brought to market by our 50+ strong interdisciplinary team of physicians, data scientists, AI experts, software engineers, regulatory specialists, and commercial teams.