PMcardio Featured on ‘This Week in Cardiology’: The Shift from STEMI/NSTEMI to OMI

We are thrilled to share that Powerful Medical’s PMcardio, affectionately known as the Queen of Hearts, was featured in the October 11th episode of the “This Week in Cardiology” podcast.
We are thrilled to share that Powerful Medical’s PMcardio, affectionately known as the Queen of Hearts, was featured in the October 11th episode of the “This Week in Cardiology“ podcast1. In the episode, a critical discussion took place around a major paradigm shift in the diagnosis and management of myocardial infarctions (MIs).
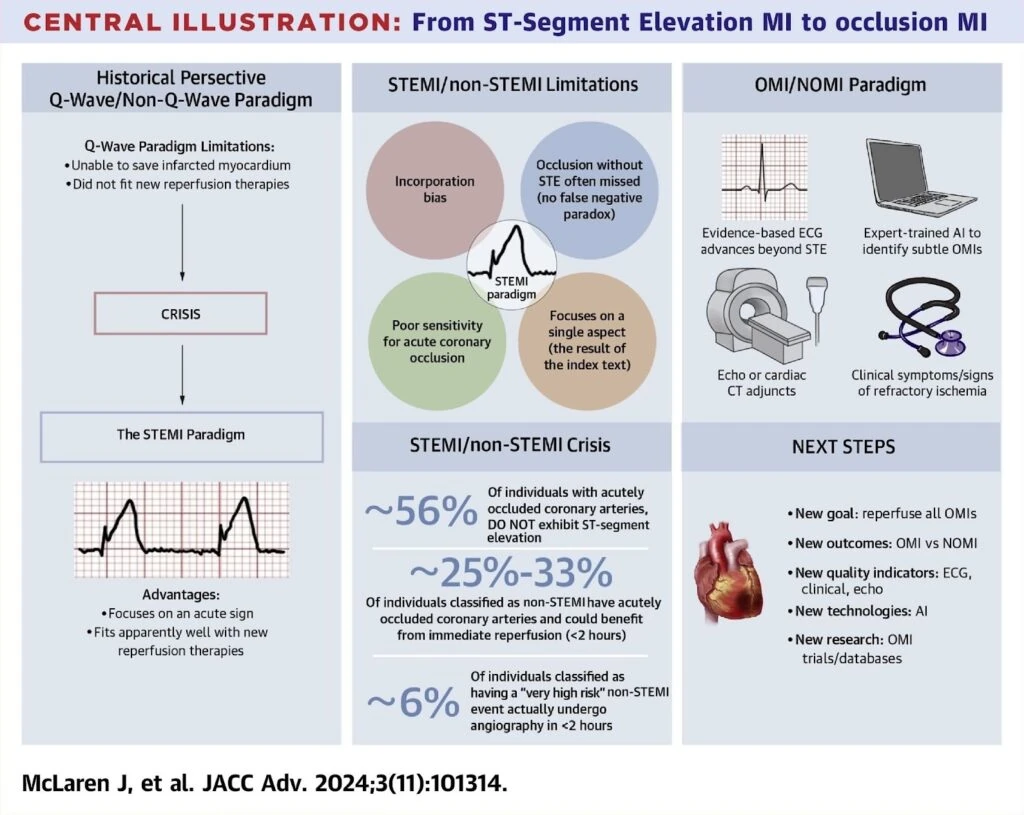
The podcast covered a state-of-the-art review published in JACC Advances, “From ST-Segment Elevation MI to Occlusion MI: The New Paradigm Shift in Acute Myocardial Infarction” by Dr. Jesse McLaren and colleagues, who argue that the long-standing STEMI (ST-Elevation Myocardial Infarction) and NSTEMI (Non-ST Elevation Myocardial Infarction) classification is outdated and, in many cases, fails to capture the true nature of a MI. Instead, the paper proposes a more precise classification: Occlusion MI (OMI) and Non-Occlusion MI (NOMI). This shift could lead to more accurate and timely treatments, preventing irreversible damage caused by delayed coronary interventions.
Why the STEMI/NSTEMI Paradigm Falls Short
For decades, the classification of MIs based on ECG findings – STEMI and NSTEMI has guided treatment pathways. If ST elevation is present, the patient is quickly sent to the Cath Lab for an emergency PCI (Percutaneous Coronary Intervention). If not, the patient is diagnosed with NSTEMI and is not considered for emergent PCI3.
However, recent evidence indicates that this long-standing paradigm has serious limitations. The authors of the JACC Advances paper argue that these misclassifications are not just academic concerns – they have real clinical consequences. Up to 30% of patients diagnosed with NSTEMI actually have an acute coronary occlusion, a condition that would greatly benefit from emergent PCI2.
A particularly sobering statistic cited in the podcast is that only 10% of patients with NSTEMI undergo PCI within 2 hours, despite a third of these patients having an acutely occluded coronary artery1. Delayed intervention in such cases results in irreversible myocardial damage. The authors further point out that 50% of patients with acutely occluded arteries do not exhibit ST elevation on their initial ECG, reinforcing the need for a new classification that better identifies the true underlying pathology of MI2. The paper proposes shifting from the traditional STEMI/NSTEMI classification to OMI/NOMI, with the core focus being on the presence of coronary occlusion rather than the ECG pattern alone2.
As the podcast host, John Mandrola MD, remarked “This may be the most important topic I have covered in a long time. Occlusion MI, not STEMI or non-STEMI. It’s time for an acute scientific revolution.”
The Role of Biases in Misdiagnosis
A key concept discussed in both the podcast and the JACC Advances paper is incorporation bias, which occurs when the outcome of the diagnostic test (the ECG) is used to confirm the results of the reference test (the angiogram)1,2. This creates a feedback loop that reinforces the STEMI/NSTEMI framework, obscuring cases where occlusion exists but is not immediately evident on the ECG.
For example, a patient with a classic STEMI undergoes angiography, and if coronary occlusion is confirmed, it is classified as a true positive. However, in cases where there is no ST elevation but coronary occlusion is later identified via angiography, this is not typically considered a false negative within the current system. Instead, these patients are often labeled as having NSTEMI, even though their coronary occlusion could have warranted emergent intervention2. This leads to mismanagement and poorer outcomes in patients who would have benefited from earlier revascularization1.
The no false negative paradox stems from this diagnostic bias, where non-ST elevation MIs with occlusion are systematically overlooked because of the reliance on ST elevation as the key marker of MI severity. Changing this paradigm is crucial for addressing this gap in cardiac care2.
Changing the Language, Changing the Outcomes
The shift from STEMI/NSTEMI to OMI/NOMI represents a critical evolution in MI management, aiming to improve patient outcomes and diagnostic accuracy. The JACC Advances paper outlines five essential changes to support this transition:
- New classification focus: Shift from identifying STEMI criteria to focusing on OMI to reduce both false-positive STEMI diagnoses and missed OMI cases2.
- Patient-centered outcomes: Medical records should reflect whether a patient has OMI or NOMI, recognizing missed occlusions as false-negative STEMI (missed OMI)2.
- Quality improvement (QI) protocols: Replace “Code STEMI” with “Code OMI,” incorporating advanced diagnostic methods like nuanced ECG interpretation, point-of-care ultrasound, and CT angiography2.
- Educational and technological advances: Learning the subtle ECG signs of OMI is challenging, and widespread educational interventions are necessary. Additionally, advancements in artificial intelligence (AI), like PMcardio, can help automate and improve the recognition of OMI. AI tools have already demonstrated greater sensitivity than STEMI criteria while maintaining specificity, making them invaluable in this new diagnostic era2,4.
- Research evolution: Transitioning to OMI/NOMI will foster new research databases and studies to improve understanding and treatment of occlusions2.
Conclusion
As the medical field moves toward the OMI/NOMI classification, there is a growing need for tools that can enhance diagnostic accuracy and speed4. This shift is crucial for improving outcomes in patients with MI, especially when early intervention can prevent irreversible damage. With its AI-driven technology, PMcardio is designed to assist clinicians in making timely, informed decisions, offering a new layer of support in identifying occlusions that might otherwise be missed4. As healthcare providers embrace this new paradigm, innovations like PMcardio have the potential to play a key role in transforming MI diagnosis and treatment, ultimately benefiting patient outcomes.
References
- 1. Mandrola JM. This Week in Cardiology [Podcast]. October 11, 2024. Available from: https://www.medscape.com/viewarticle/1001735?form=fpf
- 2. McLaren J, et al. From ST-Segment Elevation MI to Occlusion MI: The New Paradigm Shift in Acute Myocardial Infarction. JACC Advances. 2024.
- 3. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur Heart J. 2018;39(2):119-177. doi:10.1093/eurheartj/ehx393.
- 4. Herman R, Meyers HP, Smith SW, et al. International evaluation of an artificial intelligence-powered ECG model detecting acute coronary occlusion myocardial infarction. Eur Heart J Digital Health. 2023;5:123-133.
Share this article
About PMcardio
PMcardio is a CE-marked Class IIb AI medical device that interprets any 12-lead ECG — from a photo or a digital file — in seconds. It detects 50+ ECG findings, including occlusion myocardial infarction (OMI) — the acute coronary occlusions that conventional STEMI criteria miss in over half of cases. Its Queen of Hearts™ OMI model holds FDA Breakthrough Device Designation, and PMcardio is already used by 100,000+ clinicians who have analyzed more than 2.5 million ECGs.
About Powerful Medical
Powerful Medical is a medical-technology company using artificial intelligence to transform how cardiovascular disease — the world’s leading cause of death — is diagnosed. Founded in 2017, it built PMcardio, the world’s first AI medical device to detect acute coronary occlusion (OMI) from an ECG. Its research is published in the European Heart Journal – Digital Health and validated across 25+ clinical studies, and its Queen of Hearts™ model earned FDA Breakthrough Device Designation. To date, PMcardio has supported the detection of 120,000+ heart attacks across 150+ hospital deployments worldwide.