The AI standard
in cardiovascular care.
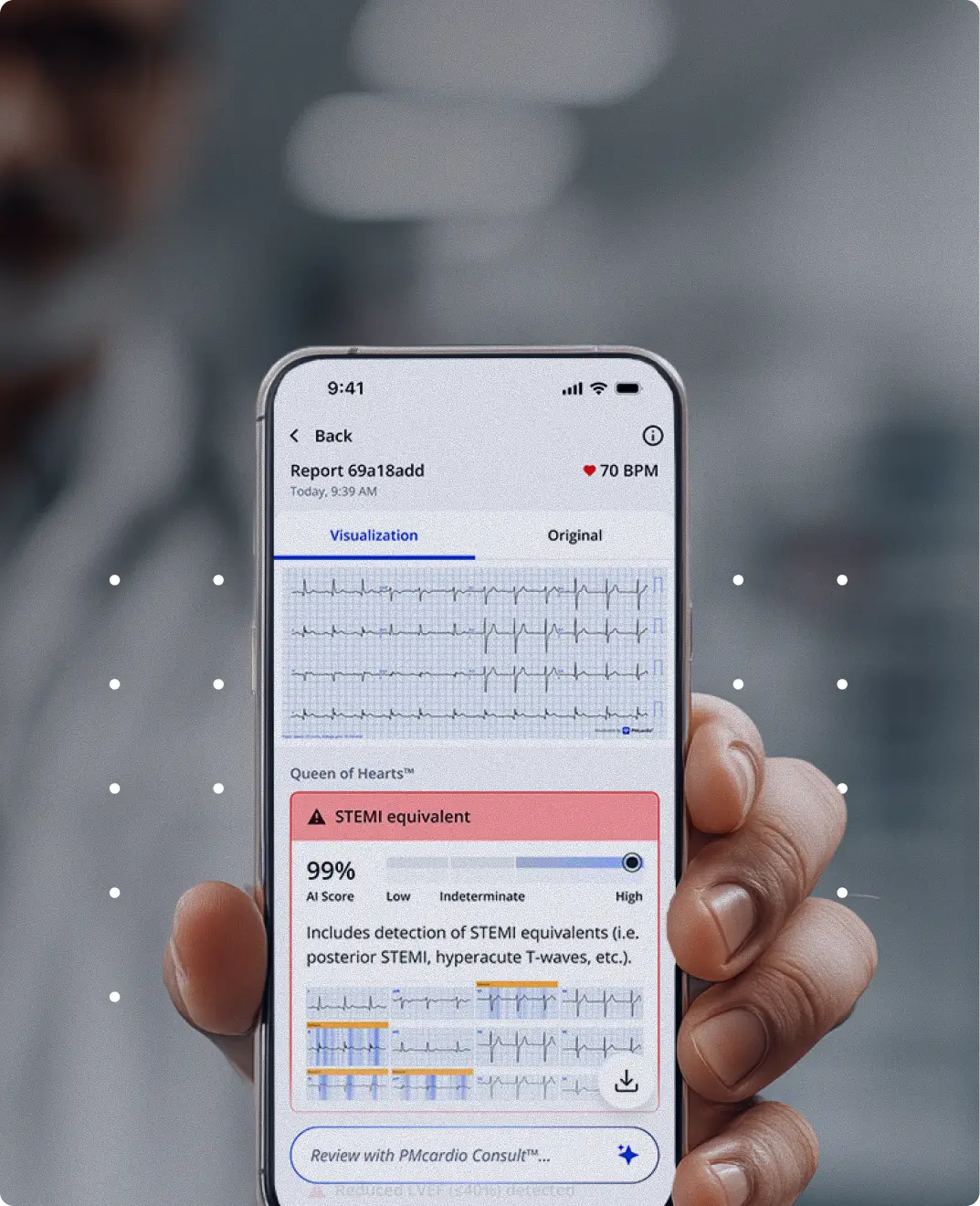
PMcardio brings instant, AI-powered ECG analysis to every clinician and every health system — from the first ECG in the field to system-wide cardiac care coordination.




across 150+ hospitals
worldwide.
1 in 2 heart attacks is misdiagnosed at the first point of contact.
PMcardio is changing that — by putting AI-powered ECG interpretation into the hands of every clinician and the workflow of every health system.
Solution Parts

Our Impact in Numbers
120kHeart Attacks Detected
- 100,000+Clinicians
Worldwide - 2.5M+ECGs
Analyzed - 25+Clinical Validation
Studies - 150+Hospital
Deployments
The latest from PMcardio








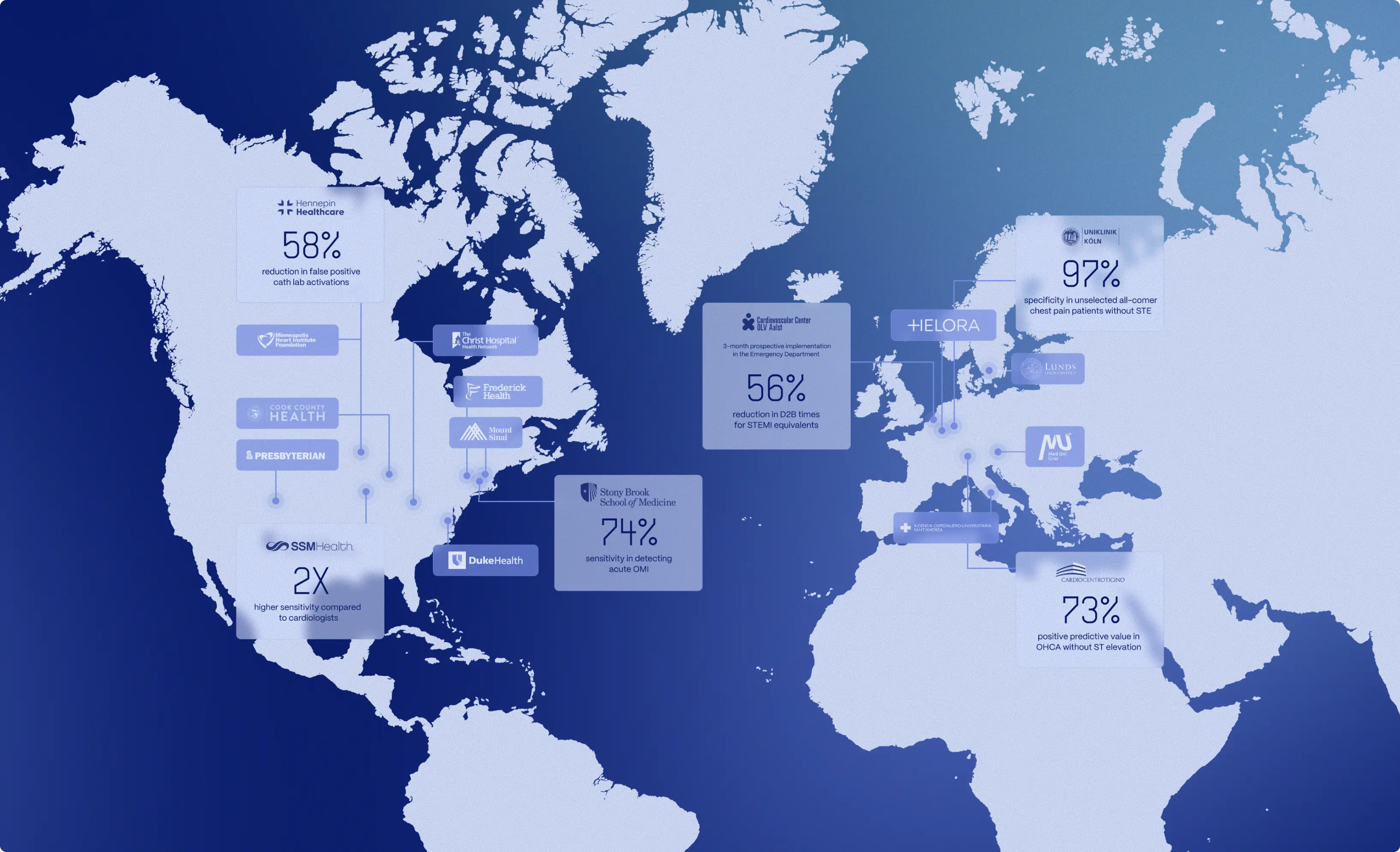
Trusted by 50+ health systems worldwide
From community hospitals to academic medical centers, health systems across three continents are using PMcardio to unify cardiac care and improve outcomes.
Podcasts
Featuring PMcardio® Queen of Hearts™
The PMcardio solution is regularly featured in the world’s largest and most respected cardiology blogs and podcasts.

FDA Breakthrough Device Designation
MDR CE Marked as Class IIb Device
“AI-Based ECG Analysis Significantly Improves STEMI Detection, Reduces False Activations.”
- ACC News Story, Oct 28, 2025

Frequently Asked Questions
What is PMcardio?
PMcardio offers CE-certified AI ECG Models that read ECGs and offers a comprehensive assessment of 50+ cardiac findings. Clinically validated in 25+ peer-reviewed studies and trusted by over 120,000 clinicians worldwide, it delivers rapid, expert-level interpretations, empowering emergency physicians, GPs, nurses, paramedics, and cardiologists to act with confidence at the point of care.
Certain AI ECG Modules are CE-marked medical devices under EU MDR and only certified for marketing in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for marketing in the USA. Not all modules and functionality of the PMcardio platform may be available in your region.
Is it safe to upload ECG images to PMcardio?
Yes, your encrypted data never leaves your region. PMcardio is fully GDPR and HIPAA compliant and adheres to the strictest regulatory and security frameworks, including SOC 2 Type II and ISO 27001 certifications. For a detailed overview of compliance, data protection practices, and security protocols, visit the Trust Center.
Is PMcardio clinically validated?
Yes, PMcardio's AI ECG Modules has been rigorously validated in more than 25 independent, peer-reviewed clinical studies. Across these studies, PMcardio AI ECG interpretation outperformed standard-of-care methods, delivering:
- 2x sensitivity for early STEMI detection (often on the very first ECG)
- Up to 92% fewer false-positive cath-lab activations (JACC: Cardiovascular Interventions, presented at TCT)
- Identifies atrial fibrillation (and other arrhythmias) with 98.3% accuracy — on par with board-certified cardiologists
For more information, the latest published evidence, and ongoing RCTs, please visit the Research page.
Which ECG formats does PMcardio accept?
PMcardio accepts any commercially available 12-lead ECG — whether a single-page image or a multi-page report. For a reliable read, three things matter: the ECG must be on standard ECG graph paper (the grid where every five 1 mm squares form a heavier 5 mm square); the whole tracing must appear on one continuous grid, not split across intersecting grids; and the image should contain only that ECG's leads, with no leads from other ECGs in the frame. Fewer-lead recordings (1-, 3-, or 6-lead) are not supported.
What ECG abnormalities can PMcardio detect?
PMcardio's AI-powered ECG algorithms recognize 50+ distinct findings across four major categories:
- Rhythms & arrhythmias: Atrial fibrillation/flutter, supraventricular or ventricular tachycardia, sinus bradycardia/tachycardia
- Conduction disorders: Left/right bundle-branch block, second- and third-degree AV block
- Ischaemia & infarction: Acute ST-elevation myocardial infarction (STEMI) and STEMI equivalents
- ECG measurements: QTc, PR, QRS and nine additional measurements
Looking for the full, continuously updated list? Navigate to the Full List of ECG Findings Detected by PMcardio AI.
Is PMcardio just another AI chatbot like ChatGPT or Perplexity?
No. PMcardio's AI ECG Models are deterministic, CE-certified medical devices purpose-built for ECG interpretation, not a conversational large language model (LLM).
- Zero hallucinations: The same ECG file always returns the same diagnosis.
- Evidence-based training: Fixed model weights are derived from 4 million+ clinically labelled ECGs with matched patient outcomes.
- Independent proof: Performance has been independently validated in 25+ peer-reviewed validation studies across Europe and the U.S.
- Regulatory oversight: Post-market surveillance and quality-management systems ensure ongoing compliance with Medical Device Regulation.
Learn more about how PMcardio compares to AI chatbots like ChatGPT.
Is PMcardio more accurate than automated ECG machine reads?
Yes. In six peer-reviewed studies, PMcardio AI ECG Models have demonstrated up to 2x higher accuracy than conventional ECG algorithms used in standard ECG machines (e.g., GE Marquette 12SL, Philips, Glasgow Algorithm).
Learn more about how PMcardio compares to Conventional ECG Algorithms.
Is PMcardio free?
Yes. Start with a Free Plan that lets you analyze up to 5 ECGs per month at no cost. When you need more reports and advanced Pro features, you can upgrade to a paid subscription with:
- Larger monthly ECG quota: run as many studies as your workflow demands.
- AI explainability for STEMI: colour-coded highlights show the waveform segments driving each positive diagnosis.
- 12 validated interval measurements: instant PR, QRS, QTc intervals and more.
- 30-day report history: revisit, download, or share any ECG analysed in the past month.
Try PMcardio for free — available now on the Apple App Store and Google Play Store.
How do I get started?
PMcardio is available on iOS, Android, and web. Start free with 5 ECGs/month — no credit card required. Download it on the Apple App Store or Google Play.
Certain AI ECG Modules are CE-marked medical devices under EU MDR and only certified for marketing in the European Union and the United Kingdom. PMcardio technology has not yet been cleared by the US Food and Drug Administration (FDA) for marketing in the USA. Not all modules and functionality of the PMcardio platform may be available in your region.
Try PMcardio
for Free
Join 100,000+ clinicians already using PMcardio to detect heart conditions with AI-powered accuracy. Get instant access to PMcardio, designed for speed, simplicity, and clinical confidence.
- No credit card required
- 5 FREE ECGs/month
- Works with any 12-lead ECG image
